WELLNESS RECOVERY ACTION PLAN (WRAP)
Recovery is a principal component to a successful mental health services fit for the twenty first century and the key role of recovery focus services cannot be over-emphasized. This essay will highlight the importance of recovery; explore the conception and history of The Wellness Recovery Action Plan (WRAP); discuss a background information and assessment of a patient, various assessment tools to be used with the patient including risk assessment, symptom and rating scales; analyse the WRAP plan for the patient, justifying its risk assessment and plan; and finally discuss patient plan of care and its planning and implementation of the patient care. The Nursing and Midwifery Council (NMC) code of professional conduct directs that patient’s confidentiality and privacy should always be protected (NMC, 2015). As a result, the patient and the trust would be protected naming patient Ms Jones.
Recovery embodies the merging of various ideas including self-empowerment, personal management, rights of disability, social integration and therapy, and is undoubtedly one of the vital new focus for mental health services with support patients, mental health policy makers and other global mental health stake holders (South London and Maudsley NHS Foundation Trust , 2010).
Several authors have defined term ‘recovery’ but it remains a well contested one. Recovery has been seen as a continuing individual journey or process that is characterized by one’s own unique experience of mental disorder and the individuals understanding attached to this perception (Meehan, et al., 2008, p. 178; Provencher, et al., 2002; Kelly & Gamble, 2005, p. 246) with the possibility that the person is able to recover even if their mental disorder is not cured (Sydney West Area Health Service – Mental Health Network, 2008)
However, the definition by one of the intellectual founders of recovery management, Anthony (1993, p. 13), stands out and widely agreed:
“… a deeply personal, unique process of changing one’s attitudes, values, feelings goals, skills, and/or roles. It is a way of living a satisfying, hopeful and contributing life even with the limitations caused by illness. Recovery involves the development of new meaning and purpose in one’s life as one grows beyond the catastrophic effects of mental illness.”
According to Repper and Perkins (2003) and Slade (2009), Anthony’s description points to the fact that recovery is living a satisfied and enjoyable life which shift the focus of who has the power to define recovery from healthcare professionals to the individual. Shepherd and friends (2008) believe that mental health professionals should as a result sensitive and detach themselves from the allegation that they are trying to ‘take them over’. Nonetheless, for recovery to be effective, it requires professionals to know what it means so that together with the service user and other stake holders, appropriate interventions and support can be implemented (Shepherd, et al., 2008).
South London and Maudsley NHS Foundation Trust (2010)asserts that even that some people a recovery model, it is perhaps suitable to rather discuss recovery concepts and ideas because ‘a model’ gives the impression about an available recovery manual that a model would suggest that there is a Recovery manual somewhere that must be used to ‘fix’ people , but on the contrary, it is less so as recovery is about personalised approached.
Andresen and friends (2006) state that recovery is a process comprising elements of taking control and responsibility, finding and keeping hope, restoring a positive identity, having an optimistic life. This same view is support by South London and Maudsley NHS Foundation Trust (2010) who state that recover means living beyond illness without essentially accomplishing the eradication of the symptoms of illness; and also, the fact that recovery mean ‘social recovery’ does not necessarily mean clinical recovery known as symptoms and cure usually applied to people with long-term conditions or disabilities such as diabetes, asthma, arthritis. Moreover, recovery is a journey and therefore a period of illness does not equate to the fact that recovery has stopped, hence some people often say they in Recovery rather than Recovered. The support and involvement offered by mental health services is part of the journey of Recovery (South London and Maudsley NHS Foundation Trust , 2010).
💬
Talk directly to your writer — no middleman.
Unlike other services, our platform lets you message your writer directly. Share extra instructions, ask questions, and get real-time updates as your paper is written.
No call centres — real writers
Wilson and colleagues (2013) believe that recovery is an essential part of the path to healing and recovery from mental illness through which the person aims to regain autonomy, positive wellbeing, develop confidence, have the ability to manage their illness, and be optimistic about the future. Equally important to recovery from mental disorder is the need cope with the illness (Cook, 2005) through the use of recovery tools such as WRAP (The Wellness Recovery Action Plan) in the treatment and management of long term mental health issues (Copeland, 2005; Kennedy, et al., 2007)
Wellness Recovery Action Planning (WRAP) brainchild of Mary Ellen Copeland and others who have themselves experiences mental health problems and looking for ways to overcome their personal mental health problems and go on to enjoy a fulfil life, goals and aspirations (Copeland, 2005; National Health Service, 2017; WRAP, 2016). According to Copeland (2005) WRAP is a self-directed and recovery system designed to assist wellness, lessen symptoms, promote personal responsibility, or improve attribute concerning life. It educates individuals about how keep themselves well, to have the capacity to recognise and monitor symptoms, and the ability to use safe, individual skills, available support, early warning signs and other strategies to cope and mitigate symptoms
Copeland (2005) further describes WRAP as a tool that can help a person’s recovery and it is guided by principles that support the recovery plan. WRAP is a methodical way for checking health, times of being unwell and times when one is distressed and uncomfortable (National Health Service, 2017). WRAP helps the user determine their own simple and Safe Wellness Tool; list things they can do every day to stay well as much as possible; recognise triggers that cause upset, identify early warning signs and develop action plans for overcoming these moments (WRAP, 2016). WRAP has five key concepts that underpins effective recovery plan namely hope, education, personal responsibility, self-advocacy and support. These five principles are geared toward empowering people with mental health issues to take responsibility about getting well, staying well, make positive decisions about their life through learning from experiences and to also look outward in terms of supporting others to get well, by so doing they themselves feel better and enhances their own quality of life (WRAP, 2016; National Health Service, 2017). Copeland (2005) also stipulates that WRAP can also be used chronically mentally patients to manage their emotional and physical issues and also can help prevent or minimize the risk of relapse.
Argument exist about the conflict between objective and scientific nature of the medical model and the subjective and personally defined qualities that underpins recovery. On one hand, the medical model focuses on the on the illness and treatment based. It would be the main support for people but, is not sufficient. On the other hand, recovery model is about personalise person-centred holistic care which promotes strength and helps avoiding deterioration (Ralph et al.,200; May,2004; Allott et al.,2002) cited in Roberts and colleagues (2007).
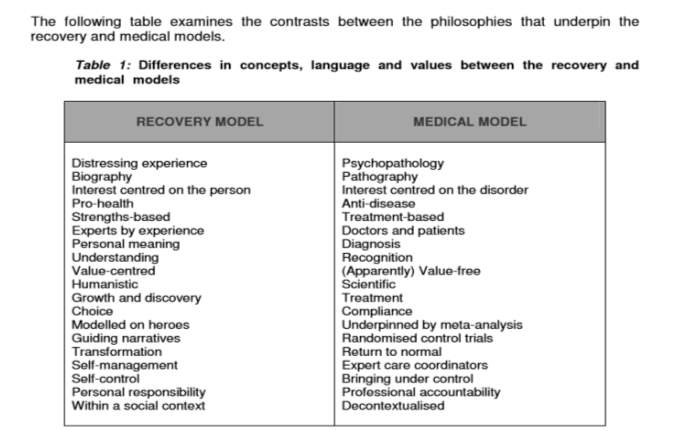 Source: Roberts and Wolfsom, 2004, p.40
Source: Roberts and Wolfsom, 2004, p.40
Patient Information
Ms Jones is a 41 years old single woman who lives in a two bedroom flat and works as a shop assistant in her community. She has been seeing her doctor for several months complaining of feeling low, she no longer enjoy work, lack of motivation, lack of sleep, loss of appetite and sometimes she experiences suicidal ideation when gets very unwell. After several tests, it was revealed she has no physical health problems. Ms Jones agreed agrees to be referred to the Psychiatrist by the GP for further assessment. She was diagnosed of major depression and was prescribe anti-depressant medication. Ms Jones was not concordant to her medication which makes her situation worse. More so, she becomes unwell and admitted that she has been having suicidal ideations. However, she mentions feeling labile mood, loneliness, isolated, stressed and anxious. She also mentions her history of depression which diagnose as stressed related in her early twenty’s. She also feels excluded from the community and even close neighbours. She has a daughter with previous partner but the relationship did not last. Ms Jones has never been in a meaningful relationship and she believes that men do not find her attractive. Ms Jones diagnosis correlates with NHS Choices (2016) and Mental Health Foundation (2017) as clinical depression. Ms Jones has also expressed concern that she does not feel well treated by the healthcare professionals as she feels they do not understand her condition and often look down on her and try to undermine her intelligence.
Assessment
During Ms Jones assessment, it was revealed that her family, friends, and the dog are her main strength, hope and support. Her day to day living was around her family and friends who’s supports her in all areas and it has serve as her coping mechanism, that is going out for tea, shopping, and walking the dog, she did mention feeling different and isolated from others. She also identifies that it rather becoming worse over the few months. she explains that she has not being in any meaningful relationship with men; the information gathered is to identify early warnings signs before things get worse.
The approach to the assessment is to inform intervention by identifying the clear target changes. Copeland (2005) stipulates WRAP has the capability to help sustain wellbeing, reduce symptoms, teaches how individuals can keep themselves properly, provide the ability to identify, monitor and use individual skills, support and other strategies to lesson symptoms, increase personal responsibility and improve the person’s quality of life. Brown and colleagues (2007) specifies that WRAP offers the opportunity to explore important ideals of recovery such as confidence, personal accountability, education, self-advocacy and support, and provides a planned progression for developing individualised WRAPs. This approach helps identifies the need of individual to motivates and empower them to takes control of their care and focus on their strength rather their weakness (Watkins, 2007).
🎓
Dissertation chapter stuck? We write every section.
Literature review, methodology, data analysis, findings, and discussion — our dissertation writers handle it all. We align with your university's exact format and provide model chapters you can reference throughout.
✓ Plagiarism-free · ✓ 100% human-written · ✓ Free revisions · ✓ Confidential
🔒 No payment to start · From $11/page
The Daily maintenance
Daily maintenance plan is the most vital part of WRAP. This is where Ms Jones baseline is identified how she is when she is well (Bentley and Walsh, 2014). The daily day to day list activity and task to maintain her wellness. These are also the things that sustain her everyday living and if she does not them it shows she is unwell. She describes herself positive and optimistic, cheerful, and outgoing person when she well. she also mentioned that her to remaining well have a good sense of wellbeing family and the friends and they are her strength. According to the strength based approach model advises that, people have strengths within themselves that speeds up recovery, it argues that families could help as main source of building on these strengths, and plays greater roles in social relationship which promote hopefulness (Huiting, 2013)
(See appendices 1)
Triggers
These are the external factors that attribute to stressed, anxious and other negative symptoms which can affect the individuals. WRAP plan is to helps the individual identify the trigger and if can be avoided or helping them to manage (Center for Mental Health Services, 2013). Ms Jones identified her triggers as Financial hardship, Worries, Lack of support from friend and family anxiety, unpaid bills and the worse is when there are occasions like Christmas birthdays and anniversary because she forgets the dates or gets them mixed up and this further stress her the more. The plan is for Ms Jones seek help from her care coordinator and family help when she starts seeing these signs. Watkins (2007) argues receiving care and direction from health professionals, brings about collaboratively working with the individuals and families and other services to recognising triggers help recovery.
(See appendices 2)
Early Warning Signs
Copeland (1999) states that there are the signs that you need recognise and act to prevent the situation getting worse. When Ms Jones did mention about her early warning signs these would make her Isolate herself, withdrawal, feeling low, hopelessness, self-neglect inadequate sleep, Lack of motivation and loss of interest. When she starts feeling this way the plan agreed is to seek support from care coordinator and emergency help line soon as possible, take medication, notify the family, and friend, have adequate rest or relaxation, and breathing exercise. She said it can also increase suicidal thought since she has been diagnosed of major depression.
Care plan
Cambridgeshire and Peterborough NHS (2011) believes that the core of the clinical and therapeutic process of care planning is developing a relationship with the service user to structure their care plan. The action plan for Ms Jones was to contact the care coordinator to arrange an appointment with Cognitive Behaviour Therapist (CBT) to support and help her manage her problem by changing the way she behaves and thinks (NHS Choices, 2016). The concept behind CBT is the fact that one can be trapped in a vicious cycle by negative ideations, thoughts and moods due to the fact that our actions, thoughts, physical sensations and feelings are interlinked. CBT therefore helps the patient deal with overwhelming issues by breaking then down into little units to help deal with the current issue instead of focusing on the past (NHS Choices, 2016).
Also for Ms Jones would be encourages to structure her day and get involved in activities to help as distraction techniques. Family and friends to help get rid of things that can be used as weapon for self-harming such are any sharp items, be encourages to stay concordant to medication and to get enough sleep and other relaxation techniques. These plans will give Ms jones her some plan to follow and work towards to support and promote her recovery when this goes worse (Cambridgeshire and Peterborough NHS , 2011).
Crisis Plan: Nelson et al. (2014) states that WRAP identifies the unavoidability of crises in events by putting together a crisis intervention team. This view is also supported by Maller (2013) who believes that the initial thing to consider in an event is crisis planning. Maller is of the view that crisis plan in WRAP is subjective where he mentioned the overwhelming managing mechanism during crisis that can affect the capability to make right, safe and positive decisions. As shown In Ms Jones WRAP below, details of her symptoms showed that she is experiencing crisis is highlighted.
Post Crisis plan: Both Maller (2013) and Nelson Et al. (2014) again agree about the importance of tough times following crisis. Post crisis plan may include the support for Ms Jones to start a normal daily routine back at home (Nelson, et al., 2014), if she was if she was, for instance, detained under section 3 of the Mental Health Act (Legislation, 2007). Post crisis plan for Ms Jones in her WRAP could also include re-establishing relationships, paying her overdue bills and returning back to work. He WRAP planned may need to be amended to reflect her post crisis and it is best and effective this is done when she is in the process of coming out of her crisis (Nelson, et al., 2014)
Assessment tools justification
Depression is normally classified into the ICD-10 (International Classification of diseases, tenth edition) and the DSM-IV (Diagnostic and statistical manual of mental disorders, fourth edition) (American Psychiatric Association, 2000; World Health Organisation, 2010). These classifications are broken down in terms of the depression such as mild, moderate, major, bi-polar, postnatal, and seasonal affective disorder (SAD). According to Mental Health Foundation (2017), depression is described as major when it immensely affects an individual’s daily activities like happiness, eating, sleep, work, and relationships.
The most commonly used assessment tools for depression are Hamilton Depression Rating Scale (HDRS), Beck Depression Inventory (BDI), Patient Health Questionnaire (PHQ), Major Depression Inventory (MDI) (Medscape, 2017). In the case of Ms Jones, MDI is used for diagnosis and measurement of her depression because it falls in line with both DSM-IV major depression and ICD-10 moderate to severe depression criteria. The assessment tool is to determine the patterns of behaviour, mood and suicidal ideation which Ms Jones has reported has been going on for few months correlates the assertion by Medscape (2017) that symptoms should be present every day for the past two weeks. Depression Inventory tool which consists of 10 questions with a multiple-choices.
For depression to be diagnosed as major 1 or 2 either items in the 5 of 9 items in the list should be established. Ten items are listed in the diagnostic tool with the items given a value (0-5) which totals up to a theoretical score of 0 to 50. The limit is set to 26 for a depressive diagnosis to be deemed major or severe (see the table below 1) (Bech, et al., 2001). Furthermore, the level of the severity of depression is usually dichotomized into three by PQ-9 scores(Löwe, et al., 2004). PHQ-9 score of 6-10 is regards as moderate depression which would call for an intervention low-intensity in the form of a self-directed guide based on CBT. A PHQ-9 score of 15 and above indicate the presence of major depression which can be treated with antidepressant such as selective serotonin re-uptake inhibitors (SSIR) like fluoxetine and citalopram (Kroenke, et al., 2001). Furthermore, patient can also benefit from psychological treatments such as therapy, advice and counselling, and general information about depression, its management and treatment to assist deal with their depression as directed by NICE Guidelines (NICE, 2009).
Major Depression Inventory and rating scale score
| All of the time |